How to Reduce Pre-Analytical Errors in Clinical Labs with LIS Automation
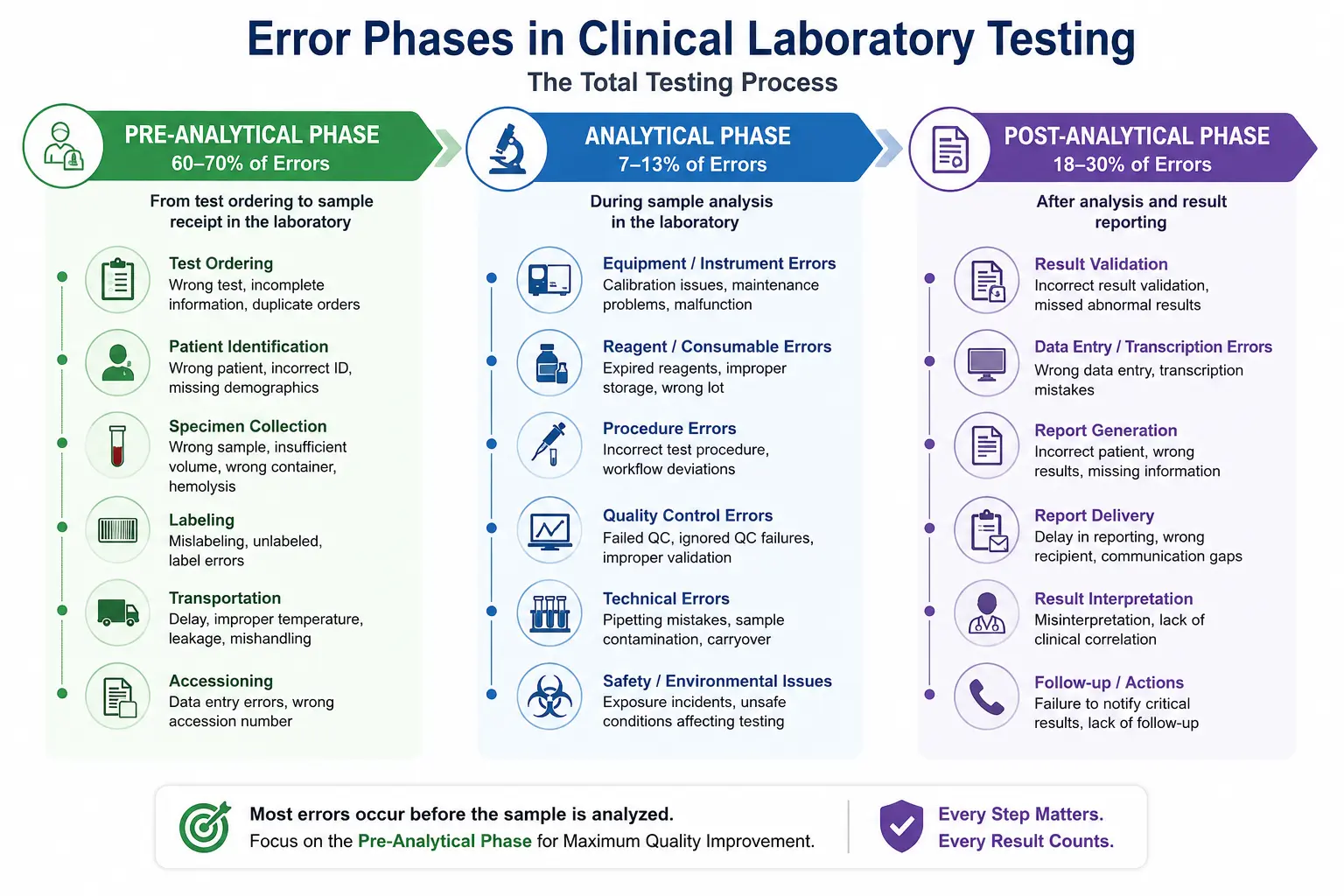
Pre-analytical errors are the single largest source of mistakes in laboratory medicine, and they happen before a sample ever reaches the analyzer. Studies published in journals like Clinical Chemistry and Laboratory Medicine consistently estimate that 60–70% of all laboratory errors occur during the pre-analytical phase the steps between test ordering and specimen testing. For lab directors, pathologists, and quality managers, reducing pre-analytical errors in clinical laboratory workflows isn’t just a quality metric; it directly affects patient safety, turnaround time, and reimbursement.
This guide breaks down the most common pre-analytical error types, why they persist even in well-run labs, and how laboratory information system (LIS) automation closes the gaps that manual processes can’t.
What Are Pre-Analytical Errors, and Why Do They Matter?
Pre-analytical errors are mistakes that occur during specimen collection, labeling, transport, and accessioning before the sample is analyzed. They differ from analytical errors (which happen during testing) and post-analytical errors (which occur during result reporting and interpretation).
Because the pre-analytical phase involves the most manual, human-dependent steps, it’s also the most error-prone. A mislabeled tube or a delayed sample can invalidate an otherwise perfectly run test, forcing recollection, delaying diagnosis, and increasing costs.
Common Types of Pre-Analytical Errors
- Patient misidentification — wrong patient, wrong tube, or wrong test ordered
- Specimen labeling errors — missing, duplicate, or incorrect labels
- Sample quality issues — hemolysis, clotting, insufficient volume, or wrong anticoagulant
- Transport and storage problems — incorrect temperature, delayed delivery, improper handling
- Order entry mistakes — duplicate orders, missing test codes, incomplete clinical information
- Timing errors — samples drawn outside required collection windows (e.g., trough/peak levels)
Each of these can trigger specimen rejection, repeat draws, and delayed diagnosis all of which erode patient trust and strain lab resources.

Why Pre-Analytical Errors Persist in Manual Workflows
Even experienced phlebotomy and accessioning teams make mistakes because manual workflows rely on repetitive, high-volume tasks under time pressure. Common root causes include:
- Manual data entry — Transcribing patient demographics or test orders by hand introduces transposition errors.
- Lack of positive patient identification (PPID) — Without barcode-based verification at the bedside, mismatches between patient and specimen are common.
- Inconsistent labeling practices — Handwritten labels or labels printed before collection increase the risk of specimen mix-ups.
- Fragmented communication — When ordering systems, EHRs, and the LIS aren’t integrated, orders can be duplicated, lost, or misrouted.
- High specimen volume and staff turnover — Labs processing thousands of samples daily have less margin for manual double-checking.
Understanding these root causes is the first step toward designing a system not just a policy that prevents them.
How LIS Automation Reduces Pre-Analytical Errors
A modern laboratory information system (LIS) automates the workflow steps most vulnerable to human error. Rather than relying on staff vigilance alone, automation builds verification checkpoints directly into the process.
1. Barcode-Based Positive Patient Identification (PPID)
Automated LIS platforms generate barcoded specimen labels at the point of collection, tied directly to the patient’s electronic record. Staff scan the patient’s wristband and the specimen label together, and the system flags any mismatch instantly. This single step eliminates the majority of misidentification errors.
2. Electronic Order Entry Integration
Instead of manually re-entering physician orders, an LIS connected to the EHR via HL7 or FHIR interfaces pulls orders directly into the system. This removes transcription errors and ensures the correct test, priority, and clinical information travel with the specimen from the start.
3. Real-Time Specimen Tracking
Automated tracking follows a sample from collection through transport, accessioning, and testing. If a sample sits too long at room temperature or misses a transport window, the system generates an alert before the delay affects results.
4. Automated Rejection Criteria
LIS platforms can be configured with rule-based rejection logic flagging hemolyzed, clotted, underfilled, or expired samples automatically at accessioning, rather than relying on a technologist to catch it manually every time.
5. Standardized Labeling Workflows
Automation enforces label generation only after positive identification, preventing the common practice of pre-printing labels a known contributor to specimen mix-ups.
6. Audit Trails and Root-Cause Reporting
Every scan, alert, and override is logged. This gives quality managers the data needed to identify recurring error patterns by shift, department, or collection site, supporting continuous improvement under CAP and CLIA quality requirements.
Manual Workflow vs. LIS-Automated Workflow
| Process Step | Manual Workflow | LIS-Automated Workflow |
|---|---|---|
| Patient identification | Verbal confirmation or wristband check | Barcode scan with system-enforced match |
| Label generation | Pre-printed or handwritten | Generated at point of collection only |
| Order entry | Manual re-entry from paper or fax | Direct EHR/HL7 integration |
| Specimen tracking | Manual logs, phone calls | Real-time electronic tracking with alerts |
| Rejection criteria | Technologist judgment, inconsistent | Rule-based, automatically flagged |
| Error reporting | Retrospective, spreadsheet-based | Real-time dashboards and audit trails |
| Turnaround time impact | Higher variability | Reduced delays from fewer recollections |
Measuring the Impact: Key Metrics to Track
Labs implementing LIS automation should track these indicators before and after rollout to quantify improvement:
- Specimen rejection rate (target: under 1–2% for most specimen types)
- Mislabeling rate per 1,000 specimens
- Turnaround time (TAT) for STAT and routine tests
- Recollection rate
- Hemolysis rate for blood draws
- Order entry error rate
Benchmarking against CAP Q-Probes data or internal historical baselines gives quality teams a defensible, data-driven case for continued investment in automation.
Expert Insights: Best Practices for Implementation
Based on established laboratory quality management frameworks (CLSI GP33 and CAP checklist requirements), labs seeing the strongest results from LIS automation typically follow these practices:
- Pilot in one department first — Roll out barcode PPID and automated labeling in phlebotomy before expanding lab-wide.
- Train on exceptions, not just the happy path — Staff need clear protocols for what to do when a scan fails or a system flag appears.
- Integrate, don’t isolate — An LIS that doesn’t talk to the EHR and instrument middleware recreates the manual gaps automation is meant to close.
- Review audit data monthly — Recurring error patterns often point to a specific unit, shift, or collection site needing targeted retraining.
- Involve nursing and phlebotomy staff in workflow design — Automation adopted without frontline input is more likely to be bypassed under time pressure.
These practices reflect real-world implementation experience across hospital and reference laboratory settings, not just theoretical process design.
Final Thoughts
Reducing pre-analytical errors in a clinical laboratory isn’t about adding more manual checks it’s about redesigning the workflow so verification happens automatically, at the point where errors are most likely to occur. Barcode-based patient identification, EHR-integrated order entry, real-time specimen tracking, and rule-based rejection criteria together address the root causes behind the majority of specimen-related mistakes.
Labs evaluating a laboratory information system upgrade should look specifically for these pre-analytical safeguards rather than assuming all LIS platforms handle them equally. Prolis LIS is one system built around this workflow, offering barcode-based specimen labeling, EHR/HL7 order integration, and automated rejection and tracking features designed to address pre-analytical error points directly. Labs researching LIS options should evaluate any vendor, including Prolis, against their specific specimen volume, integration requirements, and compliance needs before making a decision.


